















 71 / 108
71 / 108

63
Source: based on ECS 2017.
Both public and private sector facilities provide health services, whereby the Ministry of Health acts
as the main actor and provides primary, secondary and tertiary care through its facilities across the
country. Universities too are major providers of tertiary care and the private sector has increasingly
contributed to the system over recent years. The GoT itself describes the Turkish healthcare system as
“a highly regulated market with increasing private sector involvement.” (ESC, 2017)
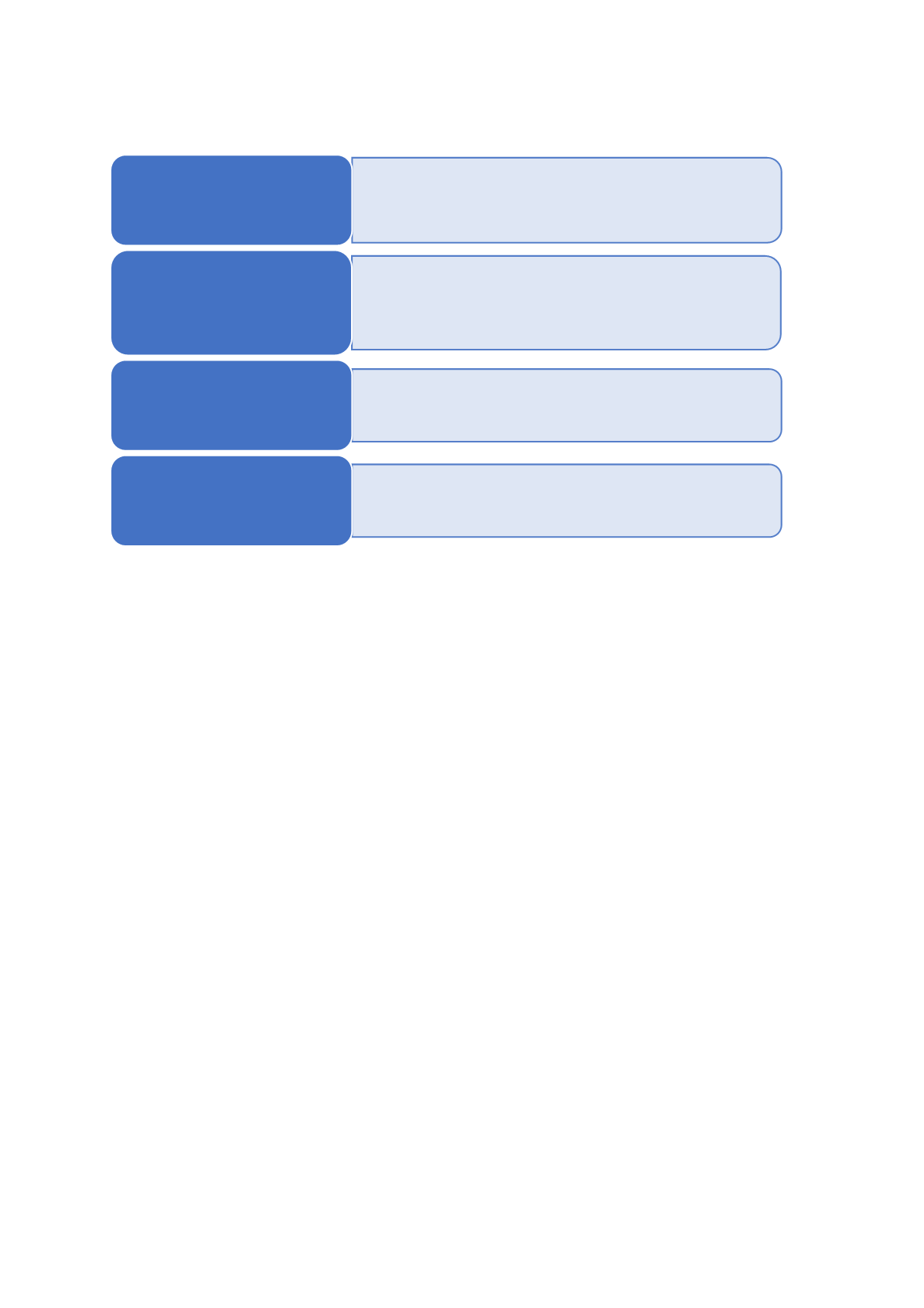
. Figure 32gives a
snapshot of the different layers of responsibility across Turkey’s health system.
A key element of Turkey’s health system is the Family Medicine program, which was rolled out
nationwide by 2010. Health centres at the primary care level were replaced by community health
centres (CHCs) and family medicine centres, in which each patient is assigned a specific doctor (WHO,
2012). Family doctors are mainly responsible for primary health care, preventive cure and guidance
on healthy life styles. This would include advice and guidance on smoking, sports, exercise and foot
diets (Giovanis and Ozdamar, 2017). For priority services (vaccination campaigns, maternal and child
health, and family planning services), family physicians are supported by Community Health Centres
(WHO, 2012).
Access to health services by Turkey’s poor
The introduction of universal health insurance in 2008 considerably contributed to achieving almost
universal health coverage, not least by reducing out-of-pocket expenditure and catastrophic health
expenditures particularly amongst the poor through their enrolment in the Green Card program.
Those previously outside the health system – “the uninsured and poor and those living in rural areas”
had 2.5 times higher catastrophic health expenditures before the implementation of the UHI in 2008
than the population in urban areas. With the introduction of the universal health insurance program
that ratio decreased to 1.3 in 2011 (Giovanis and Ozdamar, 2017). Between 2003 and 2011, the
number of Green Card holders increased from 2.5 million to 10.2 million (
Ibid.
).
• Policy is formed at this level with participation of hte Parliament, Directorate
of Strategy and Budget and MoH.
• The central government provides funding to national health care system
through budgetary allocations to public hospitals and contirbuitons to the
Universal Health Insurance Fund.
Central Government
• In addition to its role in policy formulation, the Moh is the main institution
responsible for the healthcare system; overseeing and monitoring the state of
the healthcare system.
• MoH hospitals fall directly under its mandate.
• The MoH ensures availability and delivery of pharmaceuticals, special products
and medical devices, and conducts economic evaluations to set their prices.
Ministry of Health
• Patients make monetary contributions to the SSI through compulsary premium
payments.
• The SSI reimburses public hospitals (MoH and University Hospitals) and makes
some contributions to services by private healthcare institutions.
The Social Security
Institution
• The MoH provides contributions towards the costs of private healthcare.
• Private healthcare institutions may bill up to 90% (as an additional surcharge)
which will then be provided by private insurance or out-of-pocket payments.
Private Healthcare
Services