














 98 / 148
98 / 148

Child and Maternal Mortality
in Islamic Countries
87
The MMEIG and IHME estimates show a pronounced declining trend in MMR in Indonesia
(Figure 3.29). The country has made remarkable success in improving contraceptive use from
50% in early 1990 to 62% by 2012 and skilled birth attendance more than doubled to 83% in
2012 from the early 1990 period. The total fertility rate (TFR) reduced from 3 to 2.6 between
1991 and 2012. The GDP increased fromUS $440 billion to $970 billion between 1990 and 2015.
All these social, economic and health improvement factors are likely to reduce maternal
mortality substantially between 1990 and 2015. MMR estimates by the MMEIG and IHME use a
statistical model that takes into account fertility, skilled birth attendance, and GDP/PPP, and the
low MMR estimate for Indonesia reflects the improving trends in these factors.
It should be noted here that both organizations (WHO and IHME) rely on the empirical data from
the Indonesia Demographic and Health Surveys (IDHS), which included maternal mortality
modules in the 1994, 1997, 2002-2003, 2007, and 2012 rounds. The WHO's mortality database
includes only data from the IDHS. Figure 4 shows the data sources for the IHME estimates.
Contrary to the MMEIG and IHME estimates showing a declining trend in the MMR, the estimates
from the IDHS surveys do not show a declining trend. In fact, all recent empirical data show
higher MMR estimates in recent years, compared to the model-based estimates discussed above.
The most recent MMEIG/WHO report (September 19, 2019) has revised the MMR estimate in
Indonesia to 177 in 2017 from 123 in 2015.
Trends in Child Mortality in Indonesia
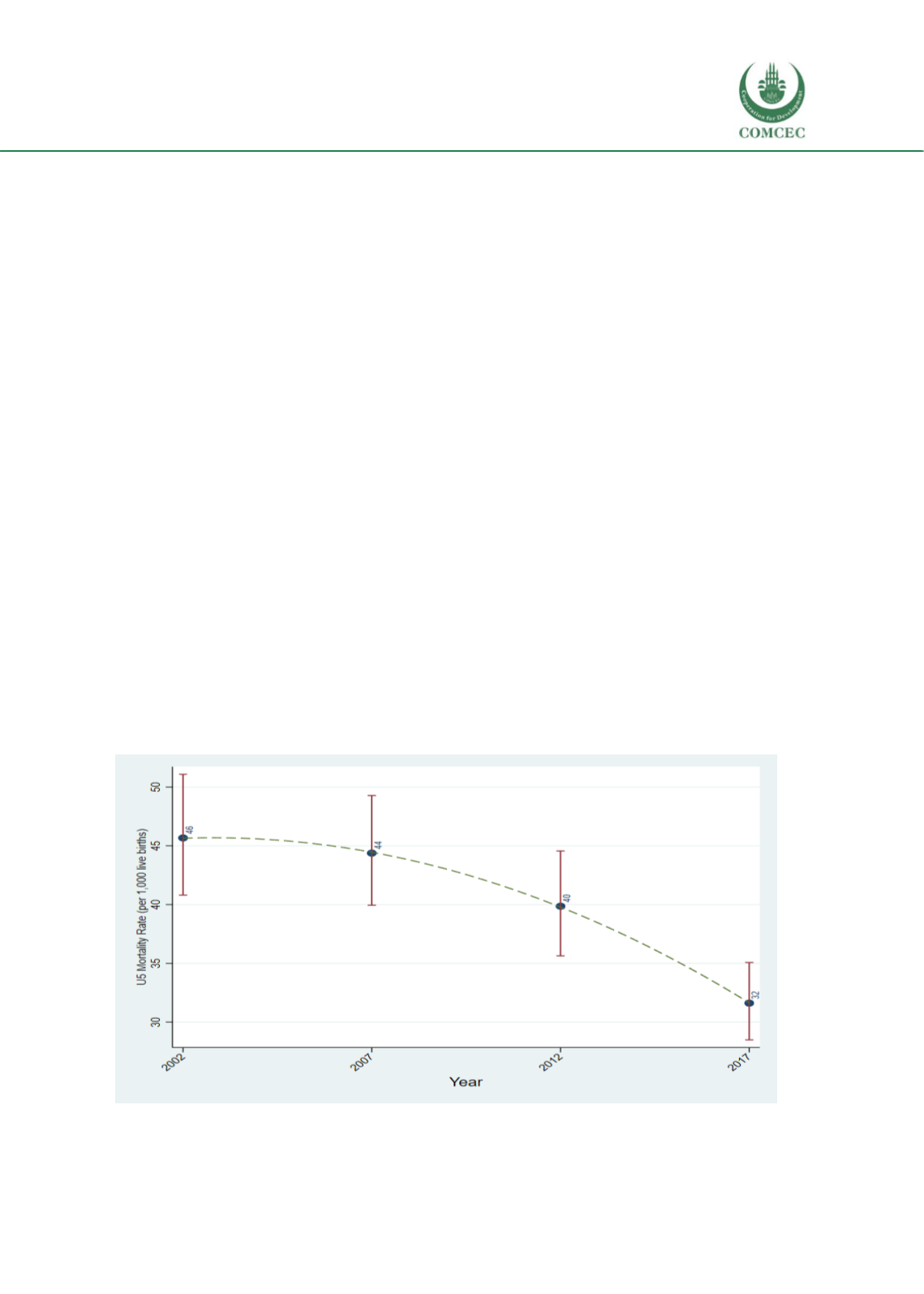
The U5MR has reduced from 46 to 32 deaths per 1,000 live births between 2002 and 2017
(Figure 3.30). The reduction of NNR was much slower: reduced from 20 to 15 deaths per 1,000
live births during the period (Figure 3.31). The U5MR reduction was more pronounced in rural
areas – from55 deaths per 1,000 live births in 2002 to 33 deaths per 1,000 in 2017 (Figure 3.32).
In urban areas, U5MR was substantially low in 2002 (35 deaths per 1,000) and remained
statistically unchanged in subsequent periods. There were no significant changes in NNMR in
urban and rural areas during this period (Figure 3.33).
Figure 3.30. Trends in U5 mortality rates, Indonesia
Data sources: Indonesia Demographic and Health Surveys