














 105 / 148
105 / 148

Child and Maternal Mortality
in Islamic Countries
94
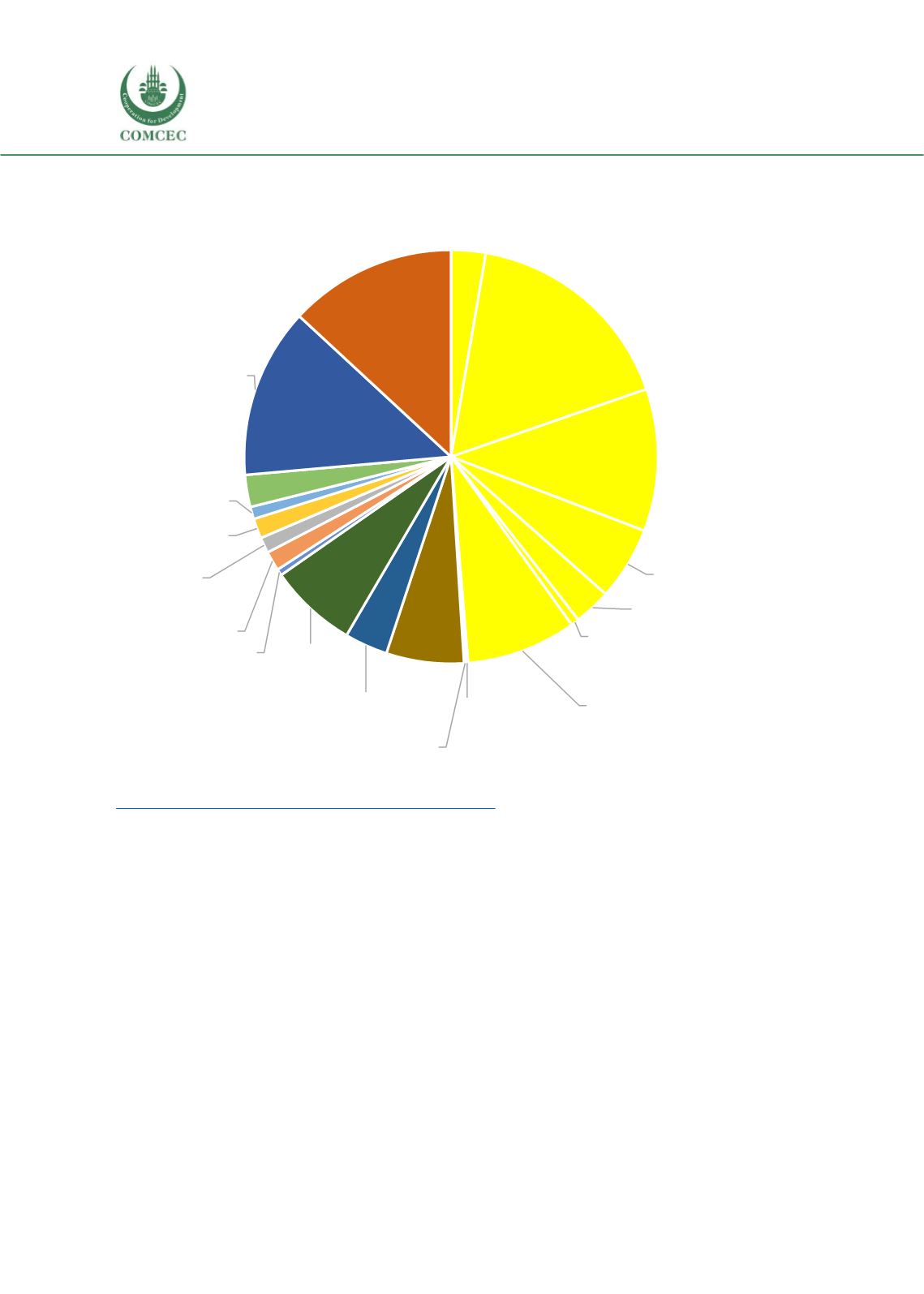
Figure 3.38. Causes of under-five deaths, Indonesia, 2017
Data source: Maternal and Child Epidemiology Estimation and Global health Observatory, available at
https://www.who.int/gho/child_health/mortality/causes/en/3.2.2. Progress in MNCH Care Indicators in Indonesia
We have presented the results of MNCH indicators from the Indonesia DHS surveys in Section-
II. In summary, overall the MNCH indicators have improved substantially in Indonesia.
However, the progress was much slower in rural areas, among poorest families and among
women with no education. As an example, the facility delivery rate is almost 23% lower in rural
areas (68% vs 91%). Only 34% women without education deliver at health facilities, compared
to 90%women with higher level of education. Among the poorest women, the delivery at health
facility has increased from 11% in 2002 to 53% 2017, but still far lower than the rate among the
richest quintile women (96%).
A similar pattern of inequity also persists vaccination coverage in Indonesia. The basic
immunization (BCG, DPT3, Polio 3 and measles) coverage rate was about 65% in 2017 and the
rates were reasonably similar in urban and rural areas (66% versus 64%). However, a large
inequity in immunization coverage was observed for wealth quintile and education level of
Pneumonia; 2,77
Preterm birth
complications;
17,45
Intrapartum-
related events;
11,42
Sepsis or
menigitis; 5,90
Other; 2,97
Injury; 0,65
Congenital; 8,83
Tetanus;…
Diarrhoea; 0,17
Diarrhoea; 6,22
Measles; 3,46
Injury; 7,08
Malaria; 0,51
AIDS; 1,57
Meningitis;…
Preterm birth
complications;…
Intrapartum-
related events;
0,98
Congenital; 2,57
Other; 13,65
Pneumonia; 13,46
Deaths among children
aged 1-59 months (49%)
Neonatal deaths