















 14 / 108
14 / 108

7
Chapter 2: Conceptual Framework
2.1
Health and development
Health was declared a human right about six decades ago. Within two years of theWHO’s endorsement
of
highest attainable standard of health
as a
fundamental right of every human being
in 1946 (WHO,
2017), the United Nations (UN) asserted health as a human right. The declaration of UN General
Assembly in Paris on December 10, 1948 stated under article 25 (1), that, “everyone has the right to a
standard of living adequate for the health of himself and of his family” (United Nations, n.d.). This right
to health also entails that the state has the legal responsibility to ensure the realization of this right;
and to put systems in place to allocate required resources provide quality healthcare accessible when
needed, and affordable and acceptable to all (WHO, 2017). From an operational point of view, this
requires a multidisciplinary system which recognises health as part of human development and
acknowledges the relationship between various socio-demographic and economic factors on the one
hand and health on the other. Socio-economic factors can result in acute and chronic deprivation from
health-related wellbeing, causing individuals and community to be disadvantaged and marginalised.
In 2015, globally about 740 million people earned less than US dollar 1.90 per day, i.e. lived in extreme
poverty. While poverty is often defined based on income status, there is a growing body of literature
that explains poverty as a social deprivation which can range from lack of income to lack of basic needs,
physical discomfort, bad relationship with others, etc. (Mabughi & Selim, 2006). Like other social
deprivations, health and poverty are intimately related. In addition to poor people having different
health outcomes compared to rich, the unequal distribution of health outcomes contributes to further
constraints and opportunities in poor peoples’ lives. For example, poor people have limited access to
healthcare, causing them to suffer from poor health outcomes, such as malnutrition and sickness,
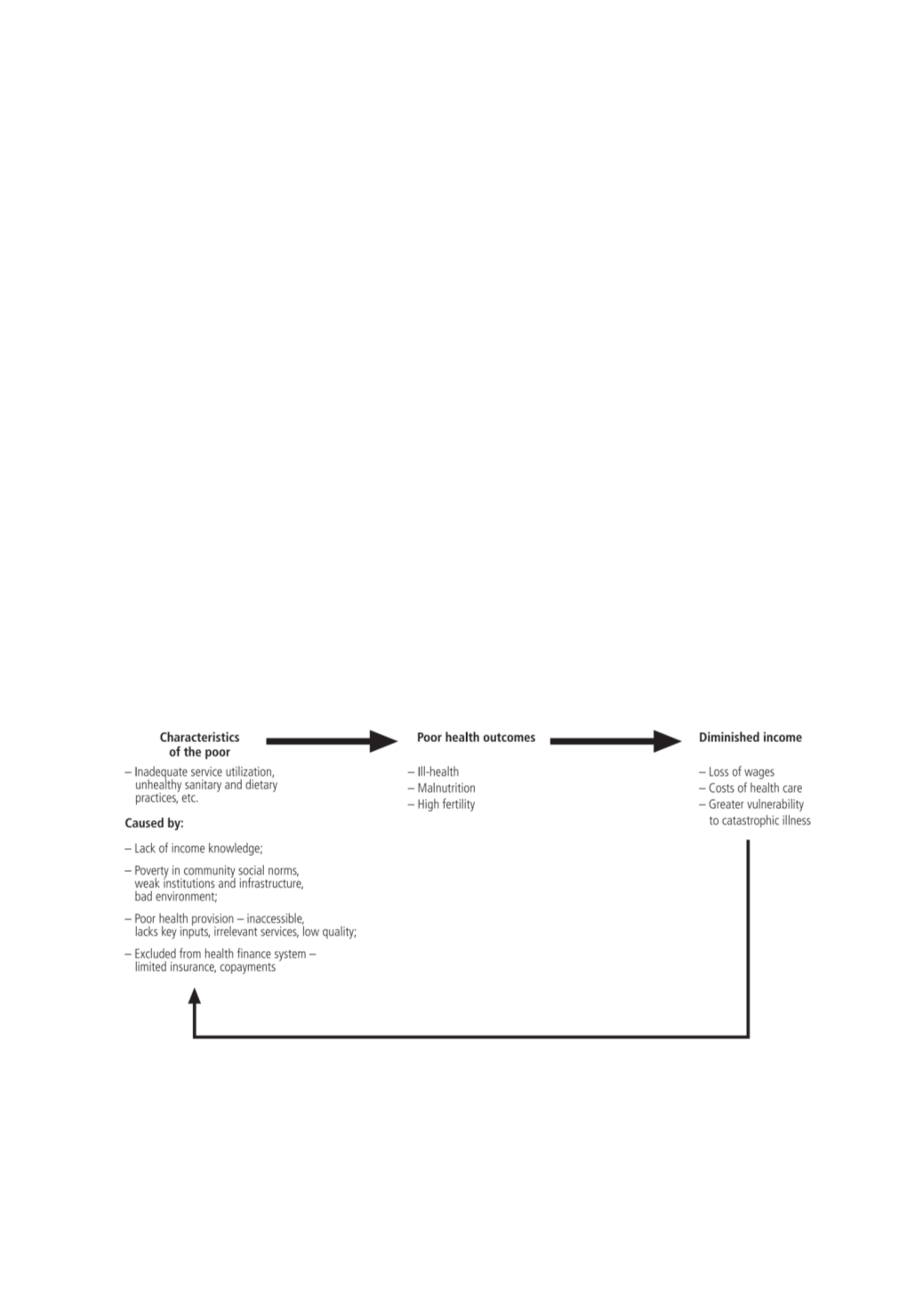
leading to reduced productivity and lower income. This can result in what is often called a
vicious cycle
,
depicted in
Wagstaff (2002)
.
Figure 2: Health and poverty cycle
Source: Wagstaff (2002)
The poverty-health cycle demonstrates two dimensions that lead to poor health outcomes for poor
people: context and access (to health). The context is related to poor living conditions, housing,
sanitation and hygiene, etc. From the health perspective, context is a risk factor for the health of the
poor. Access to health services is often restricted for the poor; either due to unavailability of services