














 124 / 164
124 / 164

Malnutrition in the OIC Member
Countries: A Trap for Poverty
COMCEC
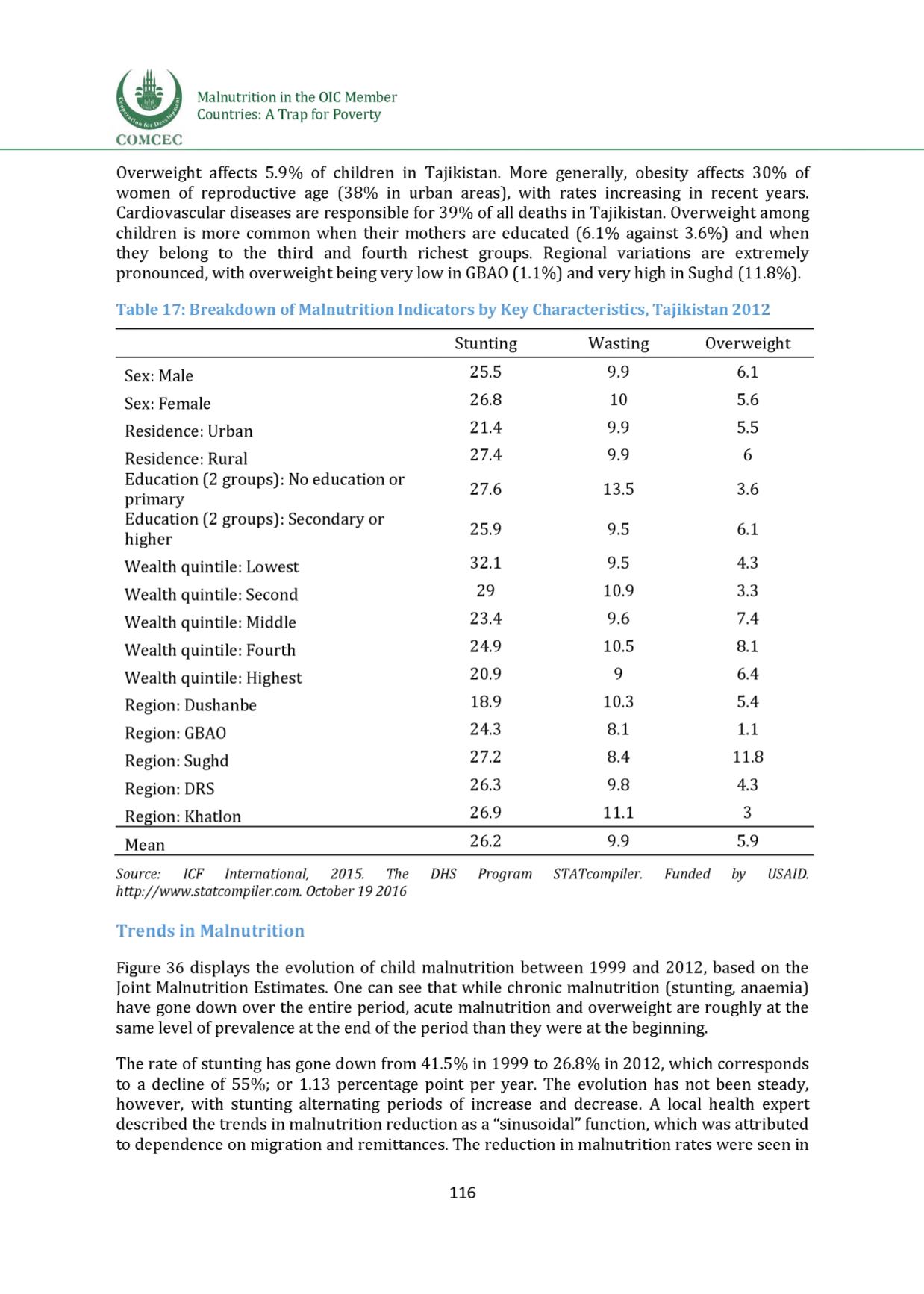
Overweight affects 5.9% of children in Tajikistan. More generally, obesity affects 30% of
women of reproductive age (38% in urban areas), with rates increasing in recent years.
Cardiovascular diseases are responsible for 39% of all deaths in Tajikistan. Overweight among
children is more common when their mothers are educated (6.1% against 3.6%) and when
they belong to the third and fourth richest groups. Regional variations are extremely
pronounced, with overweight being very low in GBAO (1.1%) and very high in Sughd (11.8%).
Table 17: Breakdown of Malnutrition Indicators by Key Characteristics, Tajikistan 2012
Stunting
Wasting
Overweight
Sex: Male
25.5
9.9
6.1
Sex: Female
26.8
10
5.6
Residence: Urban
21.4
9.9
5.5
Residence: Rural
27.4
9.9
6
Education (2 groups): No education or
primary
27.6
13.5
3.6
Education (2 groups): Secondary or
higher
25.9
9.5
6.1
Wealth quintile: Lowest
32.1
9.5
4.3
Wealth quintile: Second
29
10.9
3.3
Wealth quintile: Middle
23.4
9.6
7.4
Wealth quintile: Fourth
24.9
10.5
8. 1
Wealth quintile: Highest
20.9
9
6.4
Region: Dushanbe
18.9
10.3
5.4
Region: GBAO
24.3
8. 1
1.1
Region: Sughd
27.2
8.4
11 . 8
Region: DRS
26.3
9.8
4.3
Region: Khatlon
26.9
11 . 1
3
Mean
26.2
9.9
5.9
Source:
1CF International,
2015.
The DHS
Program STATcompiler.
Funded by
USA1D.
http://www.statcompHer.com.October 19 2016
Trends in Malnutrition
Figure 36 displays the evolution of child malnutrition between 1999 and 2012, based on the
Joint Malnutrition Estimates. One can see that while chronic malnutrition (stunting, anaemia)
have gone down over the entire period, acute malnutrition and overweight are roughly at the
same level of prevalence at the end of the period than they were at the beginning.
The rate of stunting has gone down from 41.5% in 1999 to 26.8% in 2012, which corresponds
to a decline of 55%; or 1.13 percentage point per year. The evolution has not been steady,
however, with stunting alternating periods of increase and decrease. A local health expert
described the trends in malnutrition reduction as a “sinusoidal” function, which was attributed
to dependence on migration and remittances. The reduction in malnutrition rates were seen in
116