














 117 / 148
117 / 148

Child and Maternal Mortality
in Islamic Countries
106
3.3.2. Progress in MNCH Care Indicators in Côte d'Ivoire
Skilled birth attendant was estimated at 59% in 2012 with a rich/poor gap of 56%. UN
interagency group on mortality estimation (IGME) estimates show a decrease in under-five
mortality from 152 per 1000 in 1990 to 89 per 1000 in 2017, but less progress in neonatal
mortality during the same period: from 54 to 56 per 1000 live births. The main causes of death
for under-fives in Cote d'Ivoire were malaria, pneumonia, preterm, diarrhea, and intrapartum-
related in 2014.
Overall, there exists large inequity in the MNCH indicators by socioeconomic status, educational
level of women and urban-rural residence.
3.3.3. Results from key informant interviews
In Côte d’Ivoire, we successfully interviewed 12 key informants from the Ministry of Health,
UN/WHO/UNFPA, Ministry of planning, Ministry of Finances, International NGOs, etc. Nine
participants (or 9/12 or 75%) have been in their position for 3 or more years.
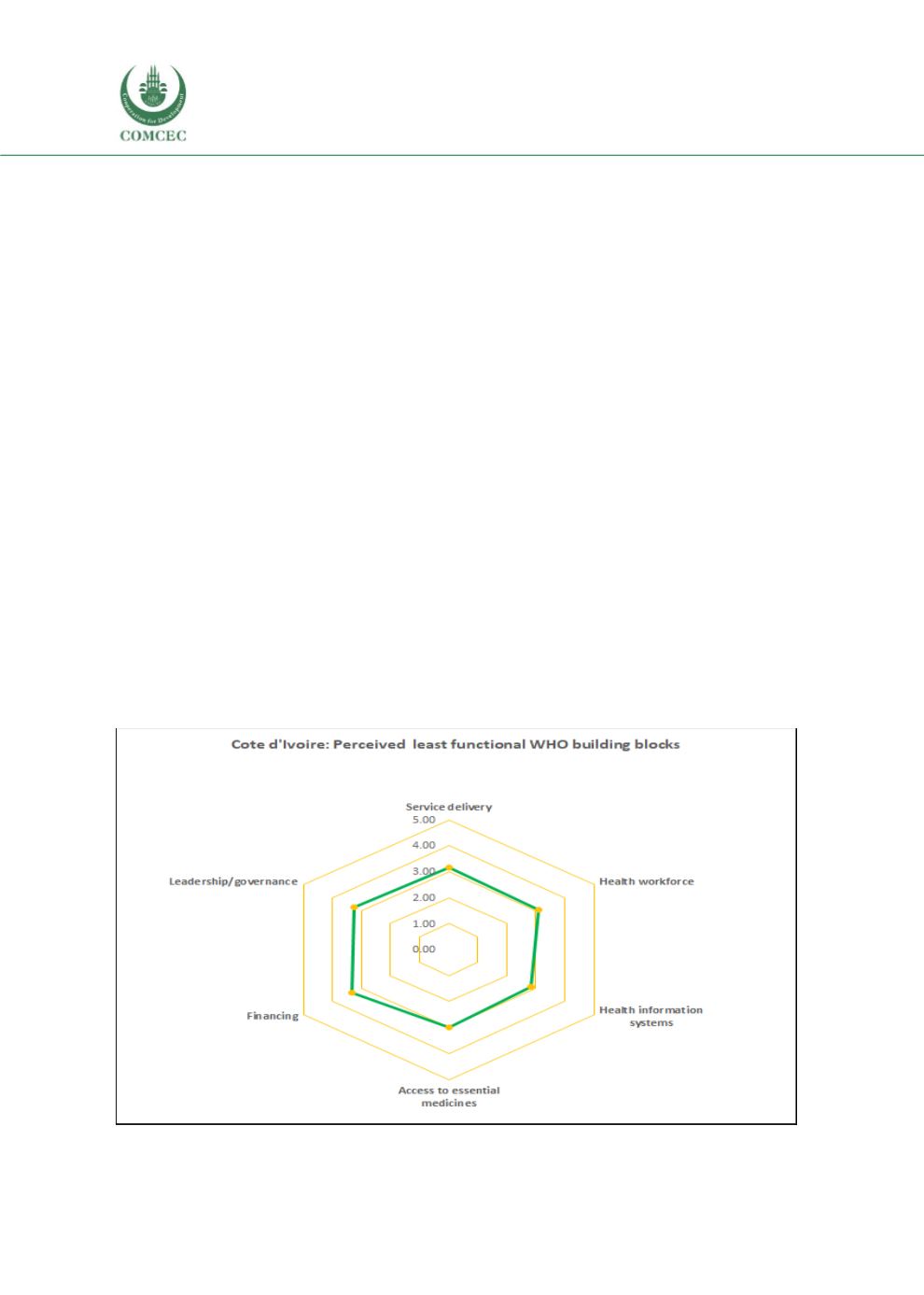
Perceived functionality of the WHO building blocks in the country
The performance of financing, leadership/governance, and service delivery were perceived
slightly poorer than health information systems, which was rated slightly better than
functioning well (figure 3.52). Access to essential drugs (average score of 3.0) and health
workforce (average score of 3.1) were perceived to be working well.
Figure 3.52. Perceived least functional WHO building blocks, Côte d'Ivoire
(1= Best functioning; 2= Better functioning; 3= functioning well; 4= Somewhat functioning; 5=
worst / not functioning)