














 21 / 148
21 / 148

Child and Maternal Mortality
in Islamic Countries
10
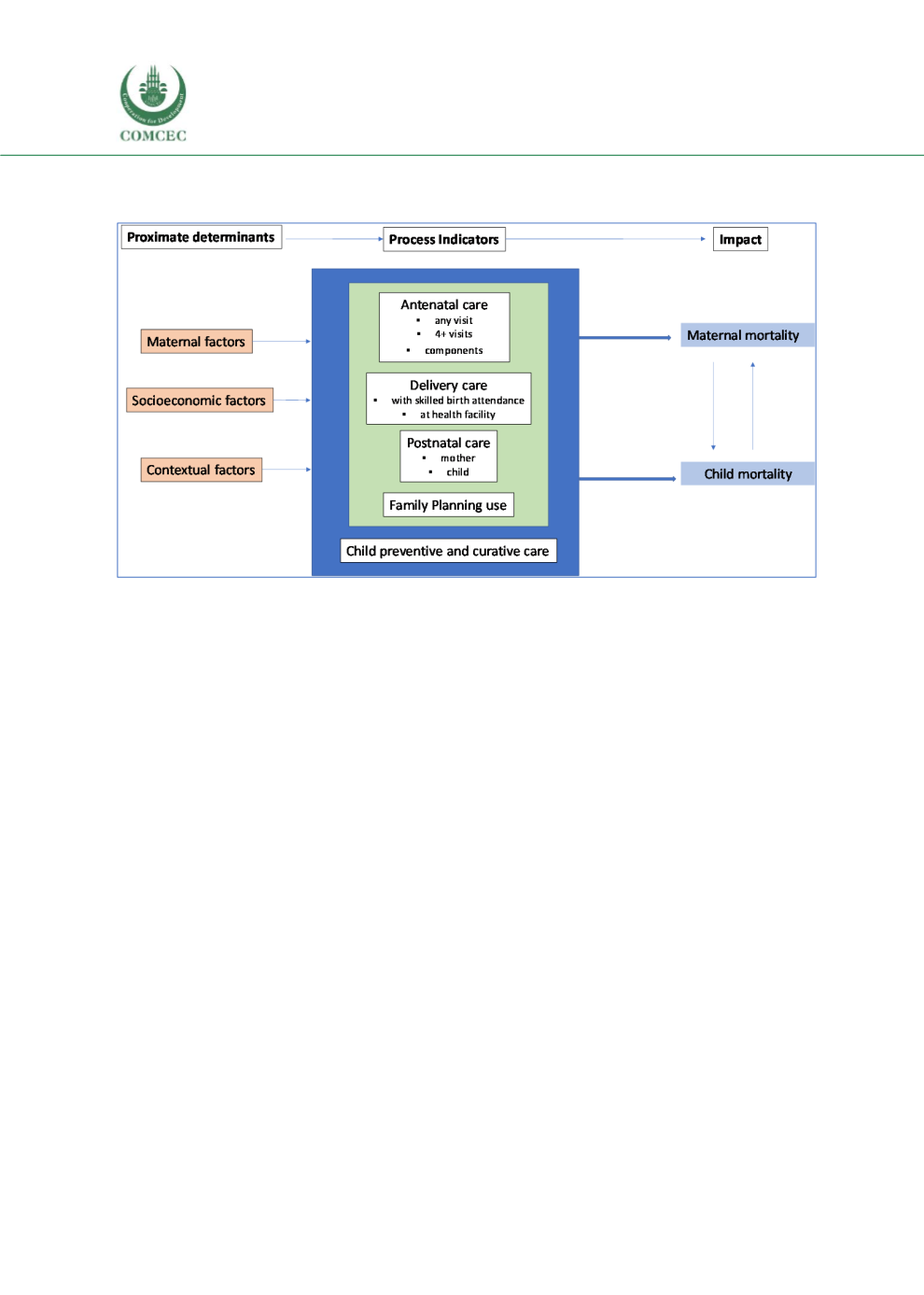
We utilized the following analytical framework to guide our quantitative analyses:
Figure 1.2: Analytical conceptual framework
We present our analytical results in the following order:
●
First, we provide the point estimates and trends of maternal mortality ratios and child
mortality rates at national level.
●
Second, we provide the results on differentials in maternal mortality ratios and child
mortality rates by selected maternal, socioeconomic and contextual factors.
●
Third, we present the results on the point estimates and trends of process indicators for
maternal mortality. These are based on the four pillars of safe motherhood initiative,
including 1) antenatal care, 2) delivery care from skilled birth attendance or at health
facilities, 3) postnatal care, and 4) family planning use. We also present the process
indicators for child mortality (child preventive and curative care) at national level.
●
Fourth, we present the results on the differentials in these process indicators of
maternal and child mortality rates by selected maternal, socioeconomic and contextual
factors.
One of our key interests are to examine the factors that are relevance to poverty alleviation
programs or targets. So, we have emphasized on three key factors: socioeconomic status,
educational level of women and urban-rural residence. In low- and middle-income countries, it
is difficult to directly measure individual and household incomes. Currently, most health surveys
in these countries assess socioeconomic status by household assets, which is commonly
presented by wealth quintiles (lowest/poorest; second/poor; middle; fourth/rich, and
highest/richest). We have examined inequity in MNCH care by wealth quintiles. In addition, we
have examined differentials of MNCH care by age of women and gainful work/employment
status of women where appropriate. The sample size for employed women are low in most
countries and the results are not presented here considering their large confidence intervals and
low reliability.